Thanks as always to Dr. Mike Silverman, Chair of the Department of Emergency medicine at Virginia Hospital Center, for these helpful updates!
Friday Night Update from the ER in Arlington, VA
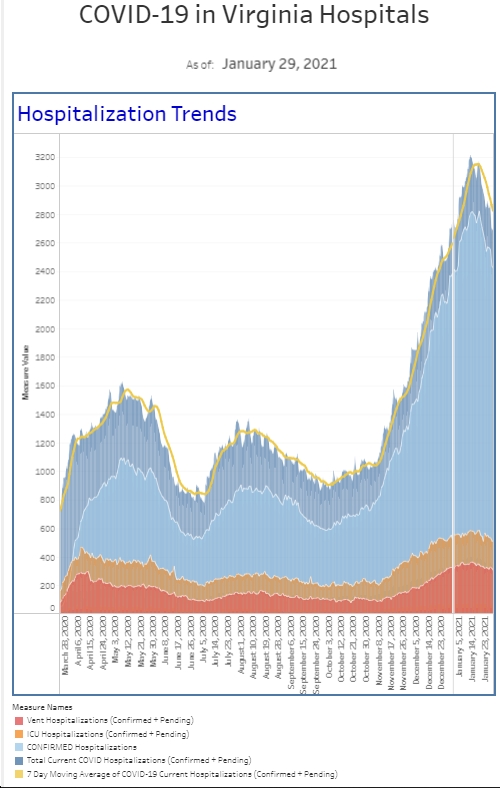
For the first time in about three weeks, I took care of a COVID patient during my shift last evening. She presented with an atypical headache like so many other Omicron patients we saw in January. No cough, shortness of breath, or fever. Omicron and the BA.2 variant are still around though cases continue to decline locally and around the country. Although I’m hearing anecdotally from friends (and their kids) that cases are increasing in colleges, we’ve continued to see a decline at the hospital. The ER is down to a sprinkling of cases a day, representing <3% of our weekly volume. It’s hard to believe that 2 months ago, new COVID diagnoses represented 30+% of our volume. Our overall percent positivity in the ER is down to about 3.2%. Two months ago it was 40%. Our biggest lull was last summer when we were well under 1% positivity and had many weeks in a row with total cases in the single digits. We’re not there yet but I hope that’s ahead for us. Our inpatient census is also down—a little over half of what it was a week ago.
Just a little bit on the BA.2 variant since I think we’ll be hearing more and more about it in the coming months. It’s spread rapidly enough to be the top variant in at least 18 countries and represents 35% of all new cases, though only about 4% of sequenced cases in the US. Danish researchers believe BA.2 is about 30% more transmissible than the BA.1 (original Omicron) but does not appear to cause more severe illness. Fortunately, reinfection with BA.2 when you just had BA.1 appears rare and was more common in unvaccinated individuals <20 years old. The average time from exposure to the onset of symptoms of BA.2 is about 3.27 day (UK publication), faster than the 3.72 days for BA.1 and 4.09 for Delta. (if you’re doing rapid tests after an exposure, this supports doing them on days 3 and 5).
Released late this afternoon are the new CDC mask guidelines that will markedly change mask recommendations at the county level. The shift focuses on severe disease and hospital capacity, aware from protecting against transmission. Previously, about 99% of the population lived in an area where masks were recommended to be worn indoors. With the new guidelines, it’s now only 28% of the population. The recommendations are based on 3 parameters—new COVID related hospital admissions over the previous week, the percentage of hospital beds occupied by COVID patients, and new case numbers per 100K population over the previous week. Low risk areas do not need masks and medium risk areas add mask use for high risk individuals (after a conversation with their doctor). Of course, anyone with symptoms, a positive test, or after an exposure should wear a mask. My gut tells me this is far from a perfect combination, but it does allow for hospital capacity to affect the decision while looking at population prevalence. (Keep in mind hospitalizations increase 2-3 weeks after we see cases rise so decision makers have to be a little anticipatory in what to expect). I think hospital employees will be in masks for a longtime and I am really curious to see how this plays out in schools and office buildings. I think we’ll continue to see peaks and valleys in case numbers so maintaining the ability to adapt to the situation is crucial. I have concerns for kids <5 as well as school age kids where vaccination rates are not high but it appears the CDC is banking on “children’s lower risk of severe illness.”
First time vaccination rates are down to 76,000 shots a day, from a peak of 1.8 million a day in April 2021. There are still large numbers of the population not vaccinated. But when they change their minds, some of them may undergo a new vaccine protocol with 8 weeks between the first and second dose. The belief is that the added time interval between the two doses could potentially extend the benefit of the vaccine and perhaps reduce the risk of vaccine associated myocarditis in the 12-39 year old age group. 8 weeks won’t be for everyone (<12 and 65+ are recommended to maintain the dosing guidelines). More info to come but I think it’s further proof that scientists are still trying to optimize care. The booster recommendations have not changed from 5 months after the second shot either,
A study out of JAMA a month ago estimated that Ivermectin prescriptions were costing insurers about $130 million annually. The overwhelming majority of these prescriptions were believed to be for COVID. Healthcare is obviously very expensive and for years, physicians have been pressured to reduce unnecessary (and costly) testing. There are many examples in the emergency department, such as reducing unnecessary imaging (radiology tests) on low back pain. If Ivermectin actually worked, this discussion wouldn’t be necessary. There’s plenty of studies already suggesting there is no role for Ivermectin in COVID, but JAMA published another study this week looking at the benefit (or lack thereof) of Ivermectin in COVID. This was a 490 patient study out of Malaysia randomizing high risk patients with mild to moderate disease to get Ivermectin or not. Unfortunately, Ivermectin did not prevent progressing to severe disease and the authors state the study does not support the use of Ivermectin for patients with COVID. I know there’s Ivermectin diehards out there. Fortunately, we do have new drugs that work (i.e Paxlovid).
Now, let’s look at vitamin supplements like zinc and vitamins D and C. While there’s lots of reasons to take vitamins, scientists from the University of Toledo analyzed 26 peer-reviewed studies from around the world, looking at 5600 hospitalized COVID patients, to see if there were clinical preventative benefits from these vitamins. Based on the data, it does appear that those “treated with vitamin D, Vitamin C, or zinc did not have a lower risk of death than those who didn’t receive vitamins.” However, vitamin D did appear to be associated with lower rates of being on a ventilator and shorter hospital stays but the authors recommend more rigorous research to confirm this finding. Those on vitamin D before getting COVID did not have a lower risk of death. One of the senior authors gave some perspective: “supplements will not offset the lack of vaccination or make you not need the vaccine.”
The Coronavirus is not done with us yet.
Science matters. Get vaccinated (or your booster). Wear a mask.
Mike