Thanks as always to Dr. Mike Silverman, Chair of the Department of Emergency Medicine at the Virginia Hospital Center in Arlington, for these superb updates. Hope you had a good/well-deserved vacation last week!
COVID, monkeypox, and polio! It has certainly been an interesting couple of weeks.
Arlington Now has used a lot of information from my Facebook posts since the pandemic began. In order to keep myself HIPAA compliant, I am going to present the facts that were reported in Arlington Now last week.. A car crashed into a very crowded restaurant in Courthouse last Friday during the dinner rush, critically injuring many people. According to the article, 8 people were transferred to the hospital for further evaluation while 6 were treated on the scene. Additionally, a fire department battalion chief was involved in an accident on the way to the scene.
The evolution of a trauma center takes place over time. It starts by having the appropriate staff and seeing the patients but then takes 1 to 2 years to go through the certification process. We started staffing our trauma center at VHC in December 2019. Many patients who sustain trauma, such as a fall from an electric scooter or a minor motor vehicle collision, are seen as routine patients in the emergency department. We have 2 levels of trauma activations, reserved for patients who have had significant mechanisms of injury (as examples: high speed MVC, fall from 3x your height) or who have significant injury based on vital signs, mental status/Glasgow Coma Scale, or physical exam). Trauma activations bring a very large response of physician/providers, nursing, and ancillary services to the patient’s bedside.
As a resident on the trauma team, I remember taking care of a drug dealer who had been shot in the chest and brought to our trauma unit. He was very lucky in that the bullet pretty much bounced off a rib, causing only a pneumothorax (collapsed lung). He got a chest tube and was admitted to the hospital. I spent a decent amount of time with him over the next week. During his hospitalization, he told me that as he rolled onto the trauma gurney, he was sure he was going to die since there were 20+ people taking care of him. It’s very scary to be a trauma patient on many levels.
Anyway, back to last Friday. I was not onsite but could not have been more proud of the care provided to the patients who came in from the Courthouse accident. Within an hour and a half, we received 3 patients who met our full activation criteria, 3 additional patients who met our modified activation criteria, and at least 2 other patients who sustained trauma. The nursing care and the collaboration with EMS, the trauma team, anesthesia, the ICU, and radiology could not have been accomplished without the last 2-1/2 years of preparing for a mass casualty incident.
Now, let’s go back to COVID, monkey box, and polio.
My initial blink on last week’s release of the CDC COVID guidelines was that they were done with COVID and declaring it over. Although I am being sarcastic, what I heard in the headlines did not make sense. As I have now read the article a few times, talked to a few others, and spent some time thinking about these new guidelines, the paper does generally make sense to me, reflects what most of us have been doing for some time, and also recognizes the poor sensitivity of the rapid antigen test.
By now, most of the population has some immunity. People are either vaccinated, have had COVID at least once, or they are vaccinated and have had COVID. So although you can certainly get COVID if you have natural immunity or immunity through vaccination, the overwhelming majority of patients are not getting critically ill. There are a small percentage of people who are immuncompromised and still at risk for severe COVID complications.
Access to testing is good and for higher risk patients, there are medications that have been shown to reduce the risk of hospitalization and death.
The key points that jump out at me are the following:
• Get vaccinated and boosted. A new booster that targets BA.4/5 should be available this fall.
• The sensitivity of rapid tests is not great. If you are symptomatic, you should repeat the test daily daily for at least 3 days (or get a PCR test). I cannot tell you how many people, friends and patients, I have come across who told me their initial test was negative and they only thought they had allergies, yet ultimately had COVID.
• If you have been exposed, wear a mask and test yourself. Early on, we had people quarantine after exposure. 2-1/2 years later, it’s not realistic to keep doing that. Exposures happen on a regular basis. For at least some period of time at the hospital, the last several months at least, we have only required testing if we are symptomatic. That makes sense to me. Routine screening that colleges that schools have done previously is likely not cost effective for an otherwise healthy population, per the CDC report. However routine screening at nursing homes, correctional institutions, and homeless shelters, may have benefit.
• If you are symptomatic or infected, you should isolate for at least 5 days and wear a mask when around others. Only after you are afebrile for more than 24 hours without the use of fever reducing medications like Tylenol and ibuprofen, and your symptoms have improved, should you venture back into the public. At this point you should wear a mask.
• If you are going to use a rapid antigen test to decide you don’t need a mask, you can start testing on day 6, and if you have 2 negative tests more than 48 hours apart, you can discontinue masking. (this recognizes the poor sensitivity of the rapid tests and also the possible rebound affect.
These are all very reasonable and honestly, what most of the medical community has been doing for several months. I think my biggest concern is for people who have rebound symptoms. This can happen whether you take Paxlovid or not. Two of my friends who had COVID about 2 weeks ago, both had rebound symptoms. One friend had several negative rapid tests over several days before he became symptomatic again and tested positive again. If this happens, you definitely have to quarantine again. (and both my friends did).
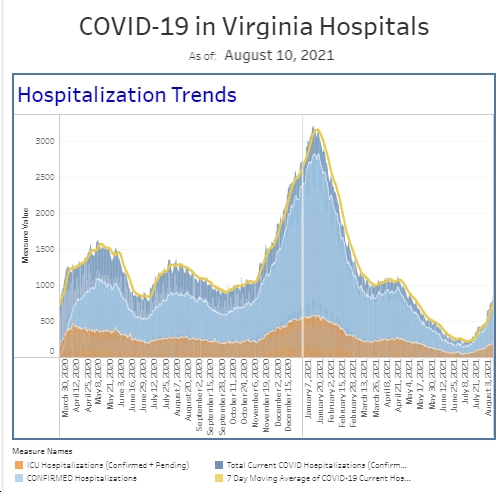
The number of reported positives that you find online is probably not the best statistic to follow anymore. Certainly, many and possibly a large percentage of people are diagnosing themselves with rapid tests and never getting counted in the total case count. Hospitals and testing centers continue to report their data. The number of patients who remain hospitalized with COVID has remained fairly constant at VHC. But over the last 4 weeks, we have seen a decrease in the [number] of emergency department patients who required our COVID isolation status. The total number of cases being diagnosed in the ER in both the symptomatic and asymptomatic population remains fairly consistent. Over the pandemic, we’ve had months where our weekly case count would go down into the single digits. That has not been the case for the last several months. We have had a steady state of patients that we diagnose each week that is not too far below the total number that we saw during our first winter peak/surge in December 2020. Unfortunately, COVID is certainly going to be with us for quite some time.
It will also unfortunately be very interesting to see what happens with monkeypox as summer ends. An ID doc told me that her their instinct was that monkeypox would not spread through schools. The numbers of cases in the area are still very low. However, following our COVID playbook, this week I participated in a multidisciplinary meeting with several specialists from throughout the hospital as well as the pharmacy, as we discussed ways to help take care of the patients that we do diagnose.
It is pretty amazing that wastewater can be studied to look for infectious disease trends. Although I’ve seen patients who had polio as a child decades ago, I have never had to diagnose a case of polio. Identifying polio in the wastewater in the New York area is certainly concerning from a public health aspect. Over and over, we have seen how routine vaccinations have saved lives around the world.
As everyone starts thinking about getting their kids back in school, I hope all of you have had an opportunity for vacation this summer. And probably like many of you, I spent some of my vacation doing some work, but certainly got in plenty of family time. It’s been a busy week since I got back to the office on Monday and I am working this weekend, and I really appreciated everyone’s comments last week when I didn’t write. Ironically, my vacation post generated more likes and comments than most of my posts. I appreciate the support.
Coronavirus is not done with us yet.
Science matters. Get vaccinated (or your booster). Keep a mask handy.
Mike