Thanks as always to Dr. Mike Silverman, Chair of the Department of Emergency Medicine at the Virginia Hospital Center in Arlington, for these superb updates!
This was a pretty good week in the ER. Volume was down a little bit which translates to increased efficiency (less time for patients waiting to see a doctor and less total time in the ER) and also allows docs and nurses to spend a little more time with patients. I had a board of medicine attorney shadow me years ago (he was a neighbor, and I can’t imagine this would take place today). At the end of his time in the ER, he said his take of my job was racing into a patient room and then racing back to my desk where I would write as fast as possible (this is before dictation and modern day EMRs). Then off to the next patient. Sometimes it feels like. I’m conscious of how much time I typically get in a room and what patients don’t typically realize is how much of their care is provided to them from my workstation. This is not only documenting the visit, but also reviewing old records, todays work up, talking to consultants or their doctors, and thinking about next steps for them.
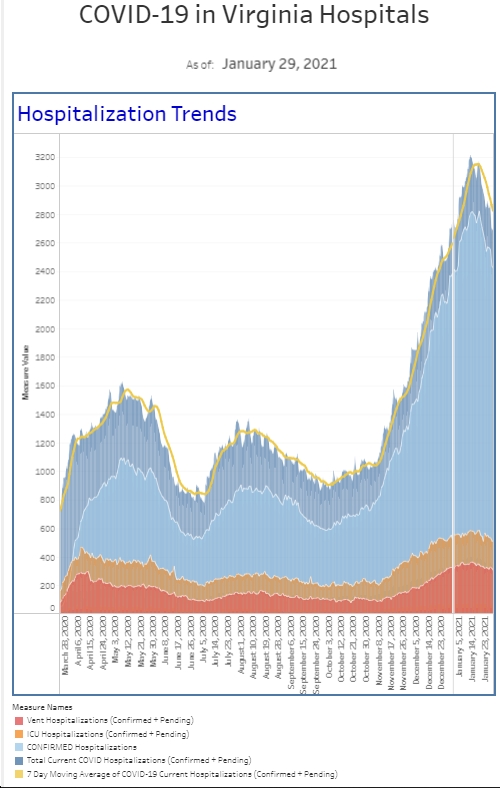
Not only was volume down a bit, but our hospital had more bed availability, so boarding was down this week, too. Our COVID numbers were also down. We’ve seen a steady decrease in the number of patients who require COVID isolation over the past month. We’ve also seen a continued decrease in the number of patients we diagnose with COVID. The number of positive tests from our “symptomatic” patient population is half of what it was two weeks ago, and the percent positive rate dropped from 30% two weeks ago to 20% this week. Our general screening positive numbers are also down by about a third from two weeks ago. Overall, we’re seeing about the same number of positives as we did before Thanksgiving. The number of people hospitalized with COVID is down a bit compared to last week and down a third compared to a few weeks ago. Our surges usually last about 2 months so maybe this one is really ending.
To close out the week, we held our annual winter/holiday emergency department party last night. This was our first formal party since the pandemic began. So why in January? As a general rule, I’m not a big fan “mandatory work fun events.” I realize they have their place and there are positives to bringing the team together. However, in a 24/7 world like the ER, where staff work weekends and nights, I want to make sure that our work event doesn’t interfere with their own personal holiday plans and parties. As a chair who gets a vote on the party, I always advocate for a winter party, so for the past decade or so, we’ve held our parties in January or February. Last night, we gathered in our ugly holiday sweaters, confusing some of the others at the venue, and had a lot of fun. There’s a lot of great reasons to work at VHC, but the team that we’ve put together is certainly among the top. (You’ll see in the attached picture, no masks. Yes, we wear masks at work, and for many of us, it was the first-time seeing people without masks, and also not in scrubs. We’re vaccinated and accessing our risk when we’re in public.)
Preliminary COVID death data from Johns Hopkins University was released this week and deaths related to COVID decreased in 2022 compared to 2021. There were about 267,000 deaths in 2022. That compares to 475,000 in 2021 and 350,000 in 2020. Despite the decrease in numbers, unfortunately COVID “will likely remain the third leading cause of death in 2022 for the third year in a row.”
I get asked a lot about whether people need another bivalent booster. Giving my personal opinion is far outside my area of expertise but I can share what I’m reading. The answer appears unclear at the moment. The booster appears to have been effective. CDC data showed that during November, hospitalizations of “adults 65+ were 2.5 times higher for those vaccinated who did not get the booster compared to those who got the updated bivalent booster.” So while older and/or vulnerable adults may benefit, there is likely much less benefit to giving additional boosters to teenagers and young adults. Ultimately, the FDA and CDC will evaluate the data and make recommendations (likely that high risk individuals will need another booster at some point). The question will then become whether it’s the current bivalent booster or will there be a trivalent booster in the near future. The XBB.1.5 strain is definitely a big wild card.
The bivalent booster made news last week when a “CDC vaccine database had uncovered a possible safety issue in which people 65 and older were more likely to have an ischemic stroke 21 days after receiving the Pfizer/BioNTech bivalent shot, compared with days 22-44.” This was announced last Friday and certainly some people immediately jumped on it as a reason to avoid vaccine. There were 130 strokes in people over 65 in that 3-week post vaccine time frame out of 550,000 shots. The signal detection meant that researchers needed to do more investigation and analysis. That review has now been completed and there does not appear to be an increased risk of stroke from the bivalent booster. Additionally, the European Union’s drug regulator did not identify any safety signals related to the vaccine.
As of earlier this month, only 39% of those 65+ have received the booster and only 16% of the population 5 and older. As people are still getting hospitalized and dying with COVID, the biggest public health opportunity may be to get those who haven’t received a bivalent booster.
There was a big study published this week looking at the impact of COVID on pregnancy. Investigators looked at 12 studies from 12 different countries, with more than 13000 pregnant patients and almost 2000 with confirmed or probably COVID. “Compared to pregnant individuals who weren’t infected, those who got Covid-19 were nearly 4 times more likely to be admitted to an intensive care unit.” Moreover, “they were 15 times more likely to be ventilated and were 7 times more likely to die.” Additionally, “they…had higher risks for pre-eclampsia, blood clots, and problems caused by high blood pressure.” Additionally, “Infants born to those with a coronavirus infection during pregnancy also had a greater risk of developing severe outcomes,” and “they were twice as likely to need treatment in the intensive care unit after birth and had an increased risk of being born preterm.”
This week, we also learned about a new superstrain of gonorrhea identified in Massachusetts that is showing signs of drug resistance. Two cases have been discovered and although the patients got better with treatment, untreated sexually transmitted infections (STIs) and having increased antibiotic resistance can lead to further medical complications—primarily worsening infections (PID, ovarian abscesses) as well as fertility issues and increasing a woman’s chance of having an ectopic pregnancy. Of course, there’s also the risk of increased transmission. Evaluating patients and treating STIs is a part of every emergency physician’s work. Treatment for gonorrhea, chlamydia, and syphilis has historically been easy but we’ve seen increasing antibiotic resistance over the last 20 years. The CDC will now have to investigate the strains found in Massachusetts.
Coronavirus is not quite done with us yet.
Science matters. Get vaccinated (or your booster). Keep a mask handy.
Mike