Thanks as always to Dr. Mike Silverman, Chair of the Department of Emergency Medicine at the Virginia Hospital Center in Arlington, for these superb updates!
Friday Night Update from the ER in Arlington, VA
I had a busy week so this should end up on the short side.
I took care of a young adult this week with moderate COVID. Vaccinated, boosted, healthy and non-smoker, with a borderline low pulse ox. They asked why “me,” when their spouse who wasn’t as healthy and just had the sniffles? And that’s part of the great unknown with COVID. Older age and risk factors clearly put you at higher risk of requiring hospitalization or dying, yet we still see young people who not only feel crummy, but may end up in the hospital. It’s an unpredictable illness, thus putting any of us at risk. Many of us, who have been COVID free since the beginning, are getting it now. BA.5 is that transmissible and makes up >80% of the current new cases. Another friend, who just got COVID for the first time, told me it really knocked him out. Both my patient and my friend were put on Paxlovid.
The doctor’s lounge is one of my favorite places in the hospital. It’s a mixing pot for all specialties and while there’s lots of conversations about routine stuff (kids, vacations, life in general), there’s plenty of medicine discussed as well. Sometimes it’s the business of shared patients. Sometimes, I’m getting an education from one specialist or another on something unrelated to emergency medicine. And often, we’re just talking about COVID—what we’re seeing, how we’re managing patients, etc…Vaccinations and Paxlovid are frequent topics. Every doc I know is vaccinated and boosted. But we’ll discuss boosters for our kids and share thoughts on the protective benefits if someone has had COVID already. This week, I had a really fun lunch conversation that included an infectious disease doc, oncologist, internist, OBGYN, and me. Spotting an infectious disease doc in the doctor’s lounge for more than a few minutes is pretty rare, so I took full advantage and we spent a lot of time talking about COVID. Paxlovid is interesting. The data seems clear that it’s beneficial for 60+ year olds. But this age group is often on medicines that preclude taking Paxlovid (or they need to stop the medicine) so there are clear risk/benefit conversations that need to occur. The data is not as clear for younger, healthier COVID patients, particularly if symptoms are mild. The rebound symptoms are likely less than 10%, but that’s not a zero risk. I had another patient who had to stop taking it because it caused severe abdominal pain.
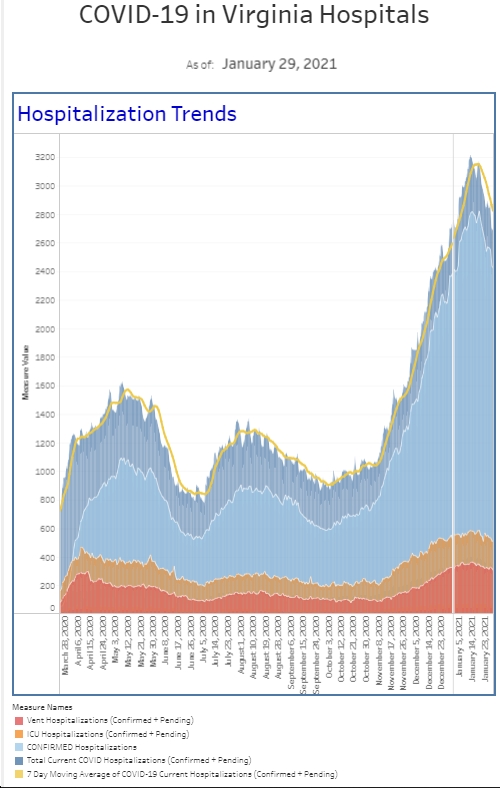
The good news is that the ER numbers looked good this week. After several weeks of climbing numbers, things flattened out or improved. The new cases we diagnosed this past week was similar to the previous week and the percent positivity was down a touch. The number of ER patients requiring “COVID isolation” protocols and the number of these patients that were admitted decreased compared to last week (after 3 straight weeks of increasing numbers). And the number of patients who are currently hospitalized is actually down 25% compared to last week.
On a public health front, it appears the government is focused on a new booster that could be rolled out this September. Both Pfizer and Moderna have promised an updated formulation by mid-September. It seems likely that a second booster will be offered to all adults one way or another, (currently for age 50+ or immunocompromised) but most likely it will be timed to coincide with the new formulation. It’s unclear at this point if a second booster will be offered to kids this fall.
Are you ready for another pandemic? The US is leading the world in Monkeypox cases with almost 5000 cases. Washington, DC has more than 170 cases making it the highest number of cases per capita in the US. Fortunately, Monkeypox does not cause the morbidity and mortality that COVID did initially, but it is contagious and can cause painful lesions. Monkeypox has not been declared a public healthy emergency (yet), but New York and California are saying it is a local public health issue. Although the LGBTQ community is seeing the highest number of cases, this will expand outside of that community. The Federal government is releasing 780,000 additional doses of vaccine, to be used by people that had close contact to others with monkeypox. I was on a call earlier this week with a handful of ER docs from around the country and one of the topics discussed was whether the emergency medicine community has the bandwidth and endurance to absorb another pandemic. (short answer—probably not). But we’ve put together our work up protocol at the hospital so we can standardize the evaluation process and continue to work on education and awareness.
Coronavirus is not done with us yet.
Science matters. Get vaccinated (or your booster). Keep a mask handy.
Mike