Thanks as always to Dr. Mike Silverman, Chair of the Department of Emergency medicine at Virginia Hospital Center, for these helpful updates!
Friday Night Update from the ER in Arlington, VA—The Holiday Edition–a day early on Thursday
That didn’t take long. The Omicron variant went [from] about 3% of sequenced samples to being the dominant version of COVID in the US. The CDC reported earlier this week that Omicron made up 73% of sequenced samples. That’s amazing transmissibility. And trust me, we’re seeing it in the ER.
Let me back up a week. I get 6 daily email reports with hospital and ER data that roll in between 5 and 7am. My ER COVID test results report last Saturday morning was eye popping in the number of new cases we diagnosed the day before. I was in touch with my chief medical officer and nursing AVP. Our COVID task force has been meeting about monthly the last few months but we held a special meeting on Monday. Although scheduled for 30 minutes, we easily filled an hour. Our staff our getting sick and furloughed. The pharmacy gave an update on monoclonal antibodies (significant shortages nationally), we discussed ED and hospital volume, supplies, etc.. It’s like being back in March 2020 except we’re almost two years in and our front-line healthcare workers are really tired.
Patient volumes are really high (I’ll get to details in a minute). My actual biggest concern is staffing. Despite vaccines and boosters, it’s very likely many people will see breakthrough infections. Doctors generally work through sickness. In the old days, it wasn’t uncommon to get IV fluids before or even during a shift, so you could work. We’ve all worked while feeling really crappy (I’ve had colleagues get diagnosed with appendicitis during their shift and yet finish the shift). However, you can’t do that with COVID. Even with mild COVID, you’re out for 10 days. The potential to have large numbers of healthcare workers taken off the job for 10 days is huge. And unlike early in the pandemic when our ER volumes fell 40-50% and we had staff looking for hours, ER and hospital volumes are back to pre-pandemic levels and we don’t have a lot of capacity left to backfill open shifts. So my biggest concern is the potential impact on absenteeism, even when doctors and nurses and other HCWs want to be at work but aren’t allowed.
COVID volume is very high. I worked today and left feeling “covid dirty” like I used to feel when COVID was new. I washed my face before I left work. I would have liked to have bathed in hand gel if possible. I changed clothes, put my gross scrubs in a bag, and couldn’t wait to get home to take a shower.
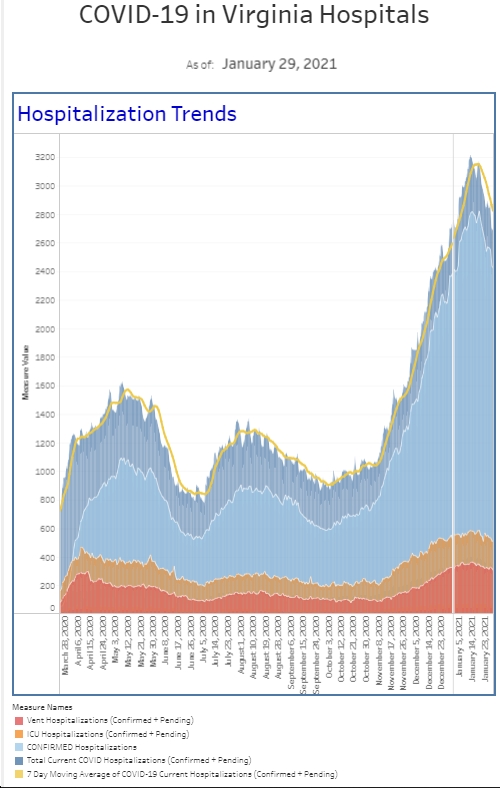
We’ve doubled the amount of “covid isolation” ordered since last week and tripled the amount from the last week of November. It’s now like the numbers seen during the second surge—January 2020. Although the admission rate has held steady at about 20% the last several weeks, the current number of patients is lower than second surge, with about half of the total number of admissions.
COVID patients make up about 25% of the patients we’re seeing on a daily basis. Now let’s look at COVID testing. Among our symptomatic patients, we had the highest percent positivity rate we’ve seen since December 2020. Our percent positive rate among our symptomatic patients was 7-10% in November and now exceeds 40% for the past week. We doubled the previous highest number of positives we’ve seen during the entire pandemic. Among all comers—we also had our highest percent positivity rate ever seen, with 50% more total positives than we’ve seen in the pandemic in any given week. Our number of positive tests went up 4 fold compared to last week and 6 fold compared to 2 weeks ago. For all tests in the ER, our November percent positive rate was 2-3%. It’s now 20% for the past week.
Omicron is everywhere. Our hospital census is up about 30% since last Friday.
This represents about 40% of our peak census of COVID patients over the last 2 years. We know hospitalizations and deaths lag 2-3 weeks behind case increases, and I do expect our hospital census to continue to increase. About 80% of our hospitalized COVID patients are unvaccinated.
It’s certainly possible that Omicron is less severe and a smaller percentage of patients will be admitted, however it’s coming from a much larger pool of patients getting sick. ER’s and hospitals are really busy. We prioritize the sickest patients. If you’re not seen quickly, it means we don’t think you’re critically ill, and that’s a good thing for you.
I’ve gotten a lot of questions about testing and monoclonal antibodies. Testing has been far less than ideal. My niece lives in England where she can order tests online daily and they arrive within 48 hours. People there are advised to test every 3-4 days and most jobs require regular testing (and then uploading results online). It’s just a part of their life and their National Health Service makes it easy (and free). My wife had an exposure at work. In a perfect world, I would have done home testing a few times over the course of a week. But neither of us could find any home tests for sale in multiple pharmacies. My local CVS told me last Sunday that they “should” be getting a delivery Thursday to be on shelves on Friday. That doesn’t cut it. Lines for public testing can take hours. And while coming to the ER sees like a good idea sometimes, coming just for a test takes up nursing time, clogs the waiting room, and will likely leave you with a 4 figure bill. My wife made an appointment for an outpatient PCR test, and fortunately she was negative at day 7, so I finally let her take her mask off.
Monoclonal antibodies (MAB) are also a challenge. There’s a national shortage of them and we don’t yet know if they work well against Omicron. It appears that Sotrovimab by GlaxoSmithKline is effective against Omicron in lab experiments, while the other MABs are not. Of course, this drug is in extremely short supply right that. With that said, MAB have seemed to help a small percentage of people avoid hospitalization if given within 10 days over the past year. (About 20 patients need to be treated with MAB to prevent 1 hospitalization) Although there’s lots of things I can do as an ER doc, MAB is an outpatient treatment and, at this point in time, with very crowded ERs, we don’t have the space to also be an infusion center. Our hospital (and I suspect most others) are expanding the capacity of outpatient infusion clinic (where you doctor can order you treatment) but I think the big issues that have to be overcome is first, whether MABs work for the Omicron variant (if so which ones), and second, if they do work, is there enough for everyone who wants them. The state controls the doses and sends them out to hospitals and infusion centers. I really think there’s a lot of opportunity for the state to step in and improve access throughout the region (Maryland had clinics run by the state). Because of limited availability of MABs, expect criteria for access to these to tighten up in the near future.
I know there’s plenty of people who just want to get back to life. The next 4-8 weeks is not the time to do it. We need people wearing masks, getting vaccinated, and getting booster shots. When ERs and hospitals are exceeding capacity, our ability to care for heart attack and stroke patients, those with pneumonia and sepsis, or those involved in traumas becomes limited. We may not have an ICU bed when you or your loved one needs it, so we need everyone to help each other.
There’s a couple of other interesting items to address. Israel was the first country to recommend booster shots and now it appears they’re recommending a 4th shot for healthcare workers and for those 60+ in age. The shot is recommended 4 months after the 3rd dose. A lot of ER docs are talking about wanting another booster as we got ours 2 months ago. Maybe 4 or 5 will be the charm.
The Pfizer data for the 2-5 year old age group is certainly disappointing. To recap, Pfizer was studying the vaccine in 6 month to 2 year old and 2-5 year olds with the 2 shot regimen. The 6 month to 2 year old’s mounted a good response but the 2-5 year old’s fell short of what the scientists were hoping to achieve (similar to 16-25 year old’s). This is science in real time. It doesn’t always work. But you go back to the drawing board and do some more studies. Pfizer has elected to go with a 3rd dose two months after the second shot which will delay data and getting EUA. I’m sure they also considered starting over with a higher dose. The good news is that there were no safety concerns in those <5 and the dosing demonstrated a “favorable safety profile.” The interim data was being monitored by an independent Data and Safety Monitoring Board found the smaller dose provided to those 2-5 years old did not achieve the expected immune response. If the 3 dose series is successful, Pfizer expects to submit data for an emergency use authorization by spring 2022.
A report out of the Imperial College of London this week, suggests “the risk of reinfection with the Omicron coronavirus variant is more than five times higher and it has shown no sign of being milder than Delta.” Additionally, the authors say, “We find no evidence (for both risk of hospitalization attendance and symptom status) of Omicron having different severity from Delta.” However, two other studies out of the UK and Scotland paint a different picture. The UK study showed that Omicron patients were 20% less likely to go to the hospital than Delta patients and 40% less likely to be admitted. The Scottish study showed that Omicron patients were 2/3 less likely to get admitted than Delta patients. This was a very large study but the Omicron patients were predominantly young and therefore less likely to get hospitalized from the get go. South Africa is reporting less hospitalizations so there’s still reason to be optimistic that the Omicron variant is less severe, but we’ll certainly have to watch the numbers.
The FDA authorized the Pfizer antiviral Paxlovid on Wednesday for patients ages 12 and up and who weigh at least 88 pounds. It’s indicated for COVID positive patients who are at high risk for severe COVID, including hospitalization and death. It needs to be taken within 5 days of the start of symptoms. It’s taken 3 tablets at a time, twice a day, for 5 days for a total of 30 tablets. Side effects include the possibility of reduced sense of taste, high blood pressure, diarrhea, and muscle aches. It’s projected to be in pharmacies in mid to late January and may have strict controls in place about who can get it. Although this should not replace the preventative benefits of vaccine, in the long run, this is a potential game changer going into 2022.
Also reported this week is that scientists from Walter Reed Institute of Research are about to announce that they’ve created a single vaccine that will work against Omicron and future variants. The Army vaccine team has been working on this for almost two years. The vaccine has finished animal trials and is completing phase 1 trials and expected to go to phase 2 and 3 trials. It’s called the Spike Ferritin Nanoparticle COVID 19 vaccine (SpFN) and “uses a soccer ball-shaped protein with 24 faces for its vaccine, which allows scientists to attach the spikes of multiple coronavirus strains on different faces of the protein.” This is definitely something to look out for in the coming months.
I had hoped to be a little more optimistic this week but it’s been a rough week for everyone in the hospital. I’ll looking forward to a few days of quiet. I hope everyone has a wonderful holiday and can safely enjoy some time with family.
The Coronavirus is not done with us yet.
Science matters. Get vaccinated (or your booster). Wear a mask.
Mike