From Gov. McAuliffe’s office:
Per Capita Caps in Senate Health Bill Would Cost Virginia $1.4 billion
RICHMOND – A preliminary analysis of the Senate’s proposed “repeal and replace” bill by the Virginia Department of Medical Assistance Services (DMAS) shows the per capita caps in the proposal would cost Virginia’s Medicaid program at least $1.4 billion over seven years.
The per capita caps in the Better Care Reconciliation Act of 2017 affect almost every population covered by Medicaid, and would cost Virginia’s program almost double the $708 million that the House-proposed American Health Care Act (AHCA) was estimated to cost over the same time frame.
“The legislation currently up for a vote in the United States Senate would blow a hole in Virginia’s budget and severely impair our ability to offer health coverage and long-term care to the people who need them most,” said Governor Terry McAuliffe. “The cuts in the current Senate bill would force states like Virginia to choose between cutting benefits for families who need them, slashing investments in other core services like education and transportation, or raising taxes. On behalf of Virginia taxpayers I urge leaders in Washington to drop this effort to push federal health care costs down to the states and work together to make coverage more affordable and accessible for every American.”
The difference between the impact of the House and Senate proposals on per capita caps lies in the “annual growth factor” – the estimation of how much costs will increase in the future over a baseline estimate of Medicaid spending. The Senate bill uses a growth factor that estimates lower growth than the House bill – and both houses use a growth factor that is arbitrary. DMAS estimates costs will outpace the growth factor of both bills; that change becomes more pronounced in later years. Provisions in the BCRA that provide safety net funds to providers and eliminate Disproportionate Share Hospital allotment reductions would not directly make up for the losses Virginia would experience from per capita caps.
These are costs associated with providing care to Virginia’s children and elderly and disabled citizens. Medicaid eligibility in Virginia is limited to low-income people who are aged, blind and disabled; pregnant women and children; and children themselves. Reducing the costs to provide services to these populations would impose difficult choices on Virginia policy-makers to reduce services or provider rates.
This DMAS analysis is preliminary and reflects the legislation that was released on Thursday, June 22nd.
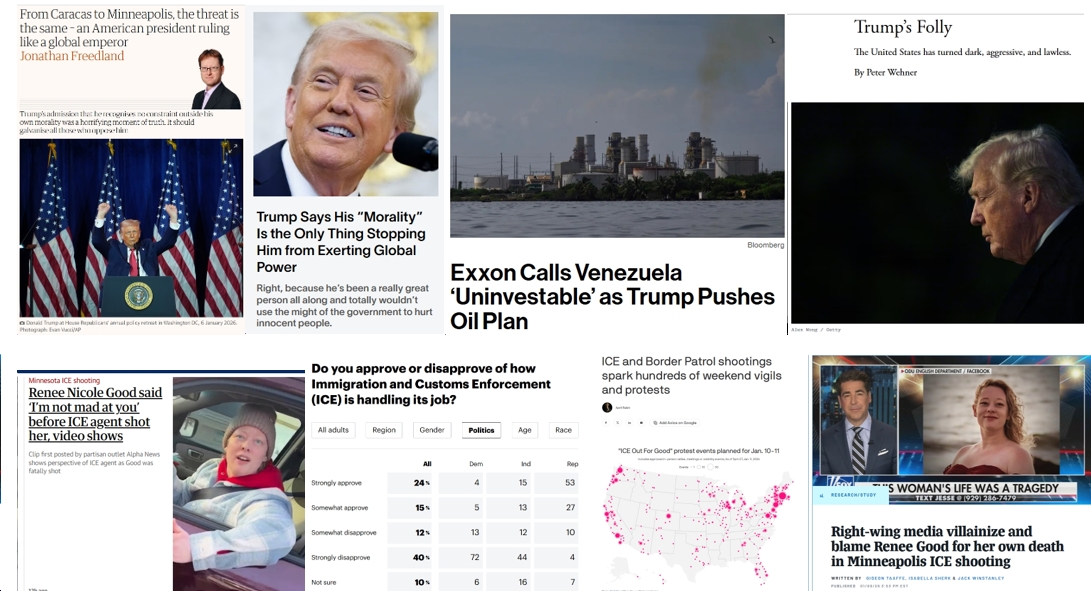
![Sunday News: “Trump Is Briefed on Options for Striking Iran as Protests Continue”; “Trump and Vance Are Fanning the Flames. Again”; “Shooting death of [Renee Good] matters to all of us”; “Fascism or freedom? The choice is yours”](https://bluevirginia.us/wp-content/uploads/2026/01/montage011126.jpg)
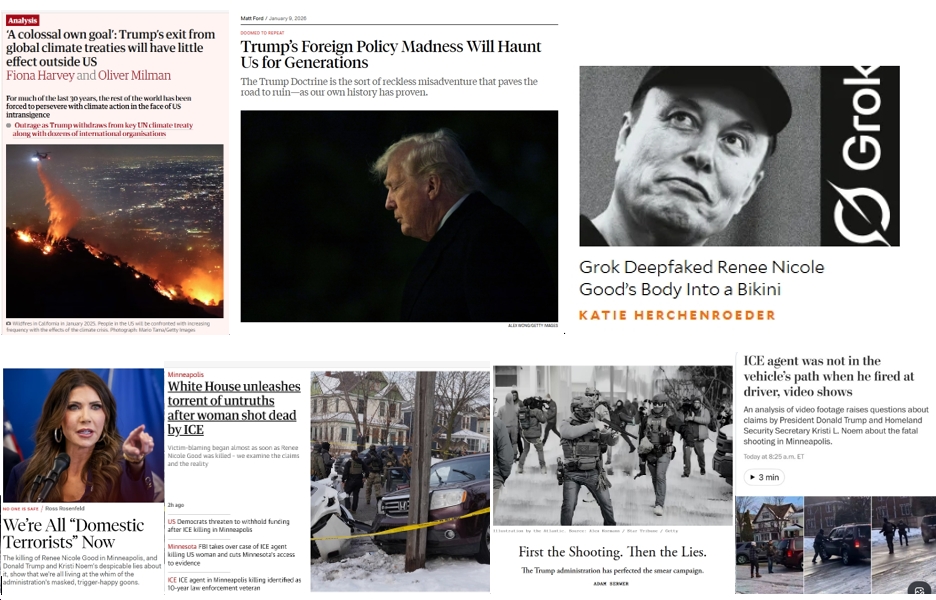
![Thursday News: “Europe draws red line on Greenland after a year of trying to pacify Trump”; “ICE Agent Kills Woman, DHS Tells Obvious, Insane Lies About It”; “Trump’s DOJ sued Virginia. Our attorney general surrendered”; “Political domino effect hits Alexandria as Sen. Ebbin [to resign] to join Spanberger administration”](https://bluevirginia.us/wp-content/uploads/2026/01/montage010826.jpg)
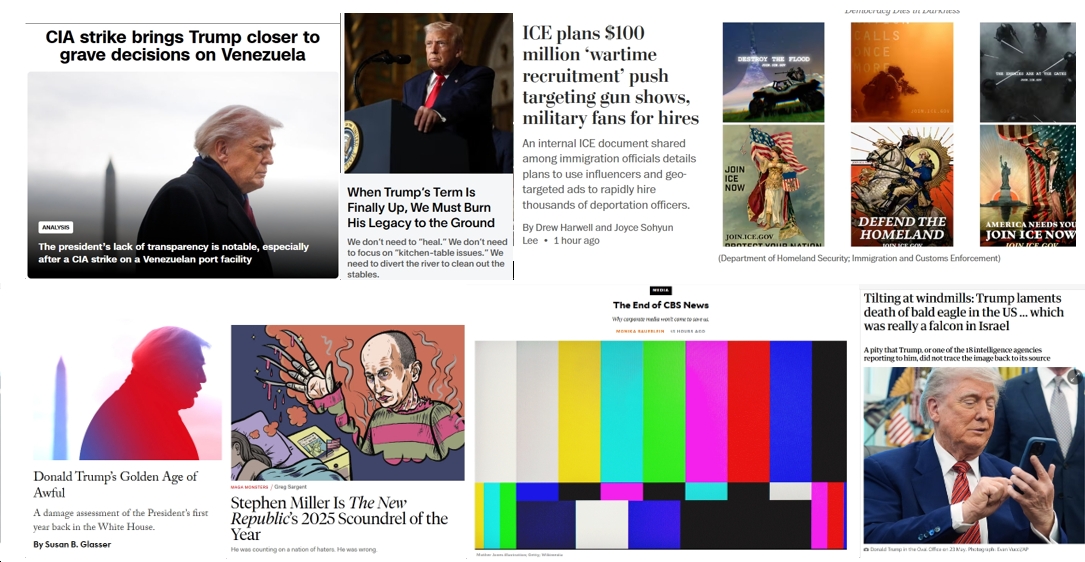
![New Year’s Day 2026 News: Full Video of Jack Smith Testimony – “The attack that happened at the Capitol…does not happen without [Trump]”; Trump/RFK Jr Make Measles Great Again; Right-Wing YouTuber Nick Shirley Definitely Not a Real Journalist; Musk Did Enormous Damage in 2025](https://bluevirginia.us/wp-content/uploads/2026/01/montage010126.jpg)