 by Dan Sullivan
by Dan SullivanThe
attacks on Medicaid expansion have begun and will intensify as the General
Assembly session gets underway. We should wait, they argue, until Medicaid is
reformed. By that argument, we should close down healthcare totally. It is service
delivery that is broken and demands reform, not the bill payers.
for procedures never performed, pharmaceutical companies that raise
prescription prices because they know insurance will cover “negotiated” costs,
insurance companies that create twisted access structures that are a barrier to
treatment and that maximize profits, companies that price medical record software to
gouge tax credits, and accountants and clerks who embezzle revenues. Yes, your
tired, your poor, your huddled Virginians yearning, no desperate, for care are
relegated to emergency rooms one way or another where a single visit might be
billed at a rate greater than the annual cost of a full year of Medicaid
preventative care. And all of this the recipients’ fault, so cut them off.
private sector to for-profit health insurance companies. Get a grip, Republicans,
you used to be the party of business but you’ve become the party of busybodies.
Medicaid should not be expanded in a
piece designed to play well with the “f&#@ you, I’ve got mine” crowd.
Seven reasons without real reason. Keep in mind, there is not a footnote or
reference in the column.
 First, it seems it took a team of renowned
First, it seems it took a team of renownedeconomists to discover that Medicaid enrollees place a low value on the program.
We are not told who, what, why or where those recipients were polled. You see,
in Virginia the vast majority of Medicaid recipients are under 19. Children are
important, but we shouldn’t be guided by their healthcare opinions. Somehow
this low valuation is twisted so that it rises from the fact that Medicaid
spending benefits large institutions, like hospitals, nursing homes, and
insurance companies, most. Well, yes, you can be certain that providers do gain
a substantial benefit from having their costs covered and not being expected to
run charities to support their going concerns. But how you measure that “most”
judgment can influence the outcome and it certainly seems that asking consumers
about service from a program that requires constant intrusive management will
affect attitudes and responses. So does resentment that other paths to access
are unavailable. This kind of survey would be an opportunity for the frustrated
to vent since no one else, including the legislators who deny them access, has
asked.
these renowned economists don’t spend time in the field. This is something you hear
consistently from people who are former clients of “free” or sliding scale
clinics but newly able to obtain health insurance under the Affordable Care
Act. They are accustomed to the kind of care and dignity afforded patients at
these facilities and at clinics like those provided by Remote Area Medical. They mistake the often disinterested and sometimes rude
treatment all of us who have always had insurance have experienced from
reception personnel in medical offices as being looked down upon because of the
insurance card they present. This is particularly characteristic of the “Doc in
a Box” medical facilities, not only at the front desk but throughout the
treatment and final farewell at the payment window. If they are going to get treated
poorly in those offices, they’ll just use their cards at the emergency room
where they don’t need an appointment and the staff is too busy to hate on them.
Medicaid patients is worse than those of “similar” patients without Medicaid.
Are you serious? Without knowing exactly what is meant by “similar” it is easy
to guess that this is cherry picked data; apples and oranges or peas and
carrots for those who made it all the way through Econ 101 or less but whose
predisposition is reinforced by such inexact comparisons. For Virginia almost
everyone between 19 and 65 who is not pregnant and meets Medicaid income limits
isn’t on Medicaid. This comparison is absolutely meaningless for Virginia.
Though, it would not be surprising that low payments to providers would affect
“service.”
disproportionate amount of non-emergency care in emergency rooms. Supposedly recent
data suggests that the Medicaid expansion has made this problem worse, not
better. Again, shape your data to your purpose. If low payments affect service
then maybe this is self-fulfilling. Poor service from non-emergency providers
may drive Medicaid recipients to emergency rooms where at least they know they
have to be seen. Come on now.
has spent time in the market at all. “Medicaid expansions tend to cause people
to replace their (often superior) and privately financed coverage with
Medicaid.” The argument all along has been that Medicaid is inferior. Now
somehow private sector insurance is only “often” superior. And one may only
imagine that the meaning of “superior” can be misleading. Does it include
affordability? Who knows? Doubtful the researcher does. But understand this:
under the Affordable Care Act, one may not arbitrarily drop coverage in the
private sector and find themselves eligible for a government insurance program
or subsidized insurance. That is not the way it works. But that is inconvenient
for the argument’s sake.
”Medicaid spending is already rapidly
increasing, threatening other state priorities. Over the past 25 years,
Virginia’s Medicaid spending, adjusted for population growth and inflation,
more than tripled. Between 1989 and 2014, Medicaid more than doubled as a
percentage of total state spending, while the share of spending going to
elementary and secondary education, higher education, and transportation has
all dropped.” – from
the RTD opinion piece
more children went without healthcare coverage and access. We are to blame the
General Assembly’s good decision to previously expand Medicaid through programs
like FAMIS for the General Assembly’s bad decisions to cut spending on
education during the economic downturn when the General Assembly was protecting
Governor McDonnell’s smokescreen of fiscal responsibility that included defunding
the Virginia Retirement System to balance the budget. And, of course it is
Medicaid’s fault that median income took a huge dive at the end of the Bush
administration; a recovery from which is almost complete due to the Obama
administration’s diligent stewardship. No, that change in relative spending was
the choice of a Republican dominated General Assembly poised now to continue
another monumental mistake having already passed on what is approaching $3 billion of our own tax money that could have expanded Medicaid, stimulated the Virginia economy, and lowered
long term healthcare costs in Virginia.
have experienced much larger enrollment and spending increases than expected. “More
than twice as many people enrolled in Kentucky as expected, more than doubling
the expansion’s cost to the state. Twice as many as expected also enrolled in
Washington, and nearly three times as many as expected enrolled in California.
In Michigan, costs are 50 percent higher than anticipated, and Ohio’s costs are
more than twice what was anticipated.”
money not state money. And if the need has been that great, that alone is an
indictment of the economy that a certain Republican administration left
for others to right. This is part of the cost of bad economic policy and
ignores the greater fact:
change with insurance coverage. Someone is going to pay for the care,
the much more expensive emergency room care, of those without health insurance.
That someone would be everyone who has health insurance that will pay the costs
of uninsured patients that is passed through to and spread among all paying
patients, insured or not.
 The final argument is even more ridiculous than
The final argument is even more ridiculous thanall others. It cries that some Virginians will lose their subsidized coverage
in the Federally Facilitated Marketplace (FFM) if Medicaid is expanded. Okay,
let’s get this straight. There is a window opportunity for those with household
incomes between 100% and 138% of the Federal Poverty Level (FPL) that Medicaid
expansion denial opens to Virginians. So we should not expand Medicaid coverage
to all below 138% FPL because Obamacare already covers some small sliver of
that population through state legislative omission. We should defend those who
are eligible for coverage under Obamacare against becoming eligible for coverage
under Obamacare at what will almost universally be less expensive than coverage
through the FFM.
is a fiscal issue. No kidding. With this one would have to agree but not with
the premise. There is no acknowledgement of what has already been pointed out:
Virginians and all Americans have some sort of access to healthcare whether
covered by insurance or not. The little game we are being asked to play here is
to pretend that denying access to preventative care will somehow lower health
care costs in the long run and that it is fine for those with coverage to pay
for those without coverage as long as we do it in the most expensive manner.
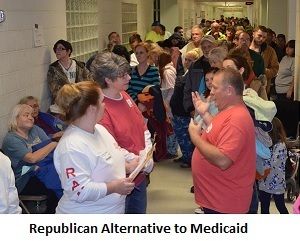
the General Assembly will be trotting out these arguments soon enough. What
will be interesting to hear is any proposal for a Republican Alternative
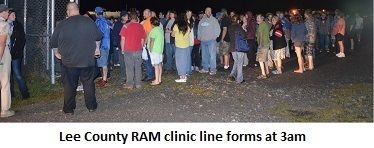
Medicaid (RAM) program. That has a nice ring to it. It can be modeled on Remote
Area Medical. In fact, it would not be surprising, since gubernatorial
candidate Rob Wittman dropped by the November Warsaw Clinic for a looksee, that
he might propose combining the two (although he hasn’t posted anything on his
website about the visit or the clinic). Maybe a public-private partnership
where the state matches the dollar value generosity of private donors and
volunteers would meet muster. At the Remote Area Medical clinics the patients
don’t complain about the service; only that it doesn’t come round more often.
theme of those opposed to expansion and the one cited first among their
arguments: recipients aren’t grateful enough for us to be bothered.
Translation: they don’t vote for us anyway, so screw them.